







Evaluation of claims-based computable phenotypes to identify heart failure patients with preserved ejection fractionSarah S Cohen et al. Pharmacol Res Perspect. 2020 Dec. Show
Free PMC article AbstractThe purpose of this analysis was to develop and validate computable phenotypes for heart failure (HF) with preserved ejection fraction (HFpEF) using claims-type measures using the Rochester Epidemiology Project. This retrospective study utilized an existing cohort of Olmsted County, Minnesota residents aged ≥ 20 years diagnosed with HF between 2007 and 2015. The gold standard definition of HFpEF included meeting the validated Framingham criteria for HF and having an LVEF ≥ 50%. Computable phenotypes of claims-type data elements (including ICD-9/ICD-10 diagnostic codes and lab test codes) both individually and in combinations were assessed via sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) with respect to the gold standard. In the Framingham-validated cohort, 2,035 patients had HF; 1,172 (58%) had HFpEF. One in-patient or two out-patient diagnosis codes of ICD-9 428.3X or ICD-10 I50.3X had 46% sensitivity, 88% specificity, 84% PPV, and 54% NPV. The addition of a BNP/NT-proBNP test code reduced sensitivity to 35% while increasing specificity to 91% (PPV = 84%, NPV = 51%). Broadening the diagnostic codes to ICD-9 428.0, 428.3X, and 428.9/ICD-10 I50.3X and I50.9 increased sensitivity at the expense of decreasing specificity (diagnostic code-only model: 87% sensitivity, 8% specificity, 56% PPV, 30% NPV; diagnostic code and BNP lab code model: 61% sensitivity, 43% specificity, 60% PPV, 45% NPV). In an analysis conducted to mimic real-world use of the computable phenotypes, any one in-patient or out-patient code of ICD-9 428/ICD-10 150 among the broader population (N = 3,755) resulted in lower PPV values compared with the Framingham cohort. However, one in-patient or two out-patient instances of ICD-9 428.0, 428.9, or 428.3X/ICD-10 150.3X or 150.9 brought the PPV values from the two cohorts closer together. While some misclassification remains, the computable phenotypes defined here may be used in claims databases to identify HFpEF patients and to gain a greater understanding of the characteristics of patients with HFpEF. Keywords: Administrative Data; Algorithm; Electronic Health Records; Heart failure. © 2020 The Authors. Pharmacology Research & Perspectives published by John Wiley & Sons Ltd, British Pharmacological Society and American Society for Pharmacology and Experimental Therapeutics. Conflict of interest statementAkeem Yusuf is an employee and stockholder of Amgen; Alanna M. Chamberlain is a coinvestigator on the REP; Sarah S. Cohen and Naimisha Movva are employees of EpidStrategies and received research contracts from Amgen, Inc for the conduct of this study. Similar articles
Cited by
References
Publication typesMeSH termsLinkOut - more resources
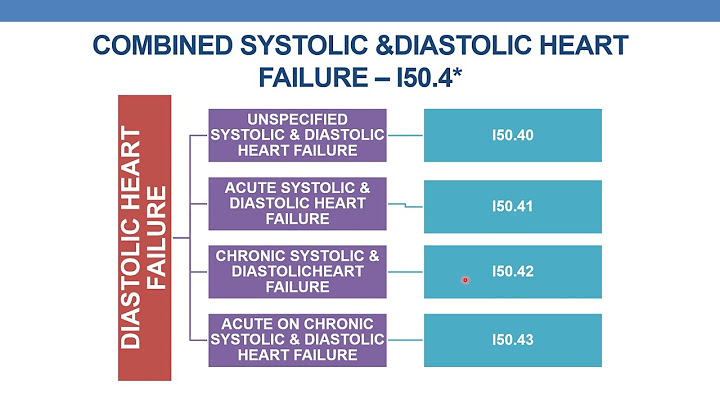
What is the ICDICD-10 Code for Diastolic (congestive) heart failure- I50. 3- Codify by AAPC.
Can you have heart failure with preserved ejection fraction?INTRODUCTION Heart failure with preserved ejection fraction (HFpEF) is a clinical syndrome in which patients have signs and symptoms of HF as the result of high left ventricular (LV) filling pressure despite normal or near normal LV ejection fraction (LVEF; ≥50 percent) [1-5].
What is another name for heart failure with preserved ejection fraction?Heart failure with preserved ejection fraction (HFpEF), also referred to as diastolic heart failure, is characterized by signs and symptoms of heart failure and a left ventricular ejection fraction (LVEF) greater than 50%.
Is congestive heart failure same as HFpEF?An even more extreme form of cardiovascular stiffening can be seen in heart failure with preserved ejection fraction (HFpEF), which comprises ∼40∼50% of elderly patients diagnosed with congestive heart failure.
|

Icd 10 for heart failure with preserved ejection fraction

Copyright © 2024 en.apacode Inc.